Better sleep is a skill. Small, repeatable moves — not perfection.
Sleep & Insomnia
A deep dive into how sleep works, why insomnia sticks, and the tools that actually shift things —
including CBT-I, 3 am rescue steps, and guides for shift workers, teens, menopause, chronic pain,
PTSD/nightmares, and sleep apnoea. UK & Scotland support links included.
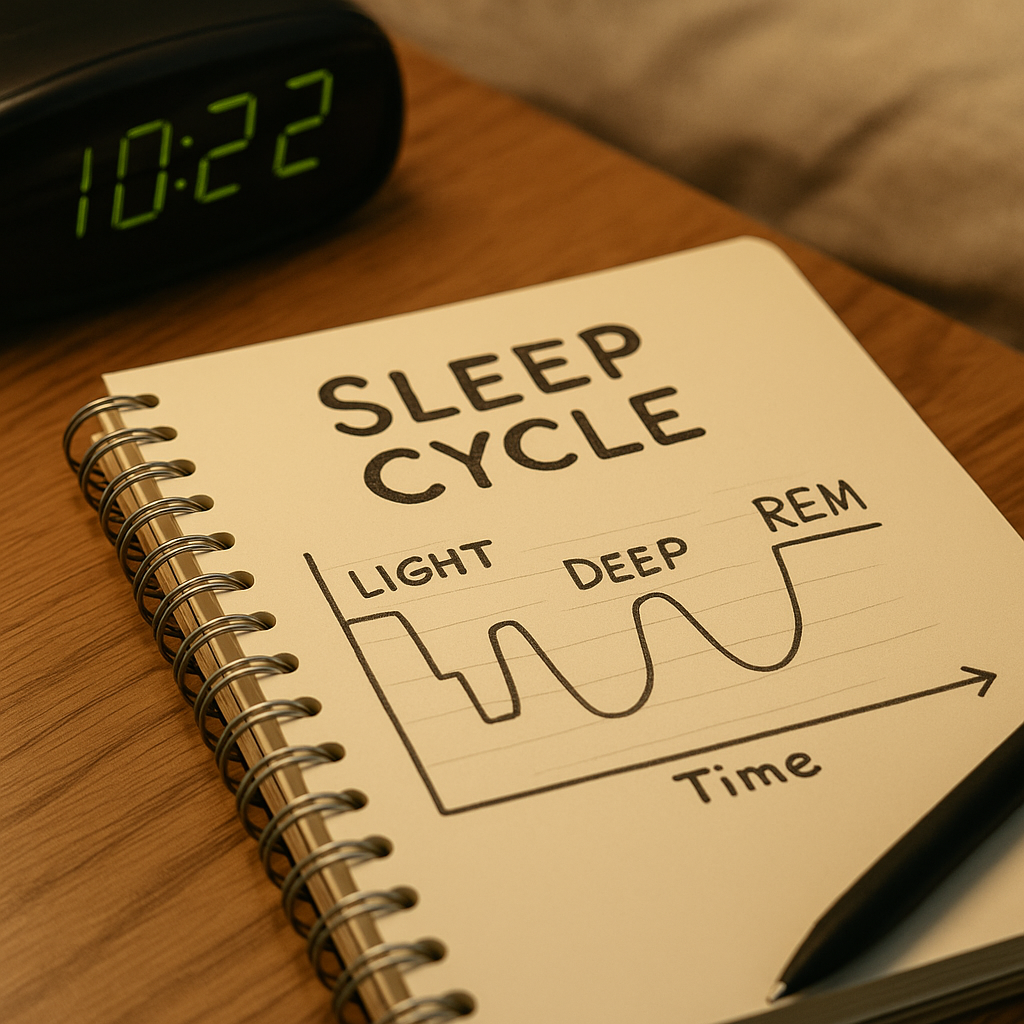
1) How Sleep Works (the useful science)
You cycle every ~90 minutes: N1→N2→N3 (deep)→REM. Later cycles = more REM.
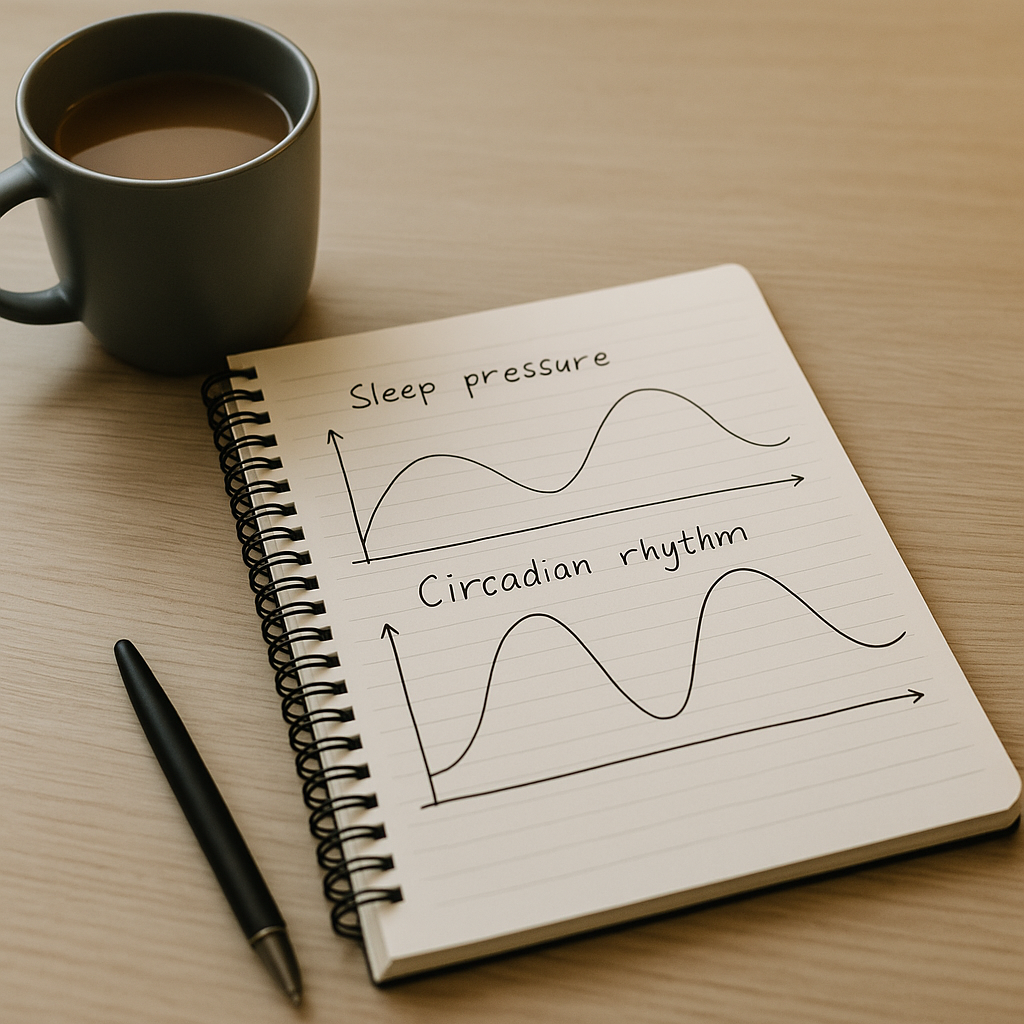
Two-process model
Sleep pressure (adenosine): builds while awake; caffeine blocks its receptors temporarily.
Circadian rhythm: the body clock sets a “sleep gate” at your usual time; morning light advances, late light delays.
Key chemicals
Melatonin: darkness signal; rises 1–2 h before habitual sleep. It nudges timing, it doesn’t “knock you out”.
Orexin (hypocretin): wake drive; steadies alertness. Loss = narcolepsy.
GABA: main calming transmitter (enhanced by many sleep meds).
Cortisol: should peak in the morning; chronic stress can keep it high at night.
Why insomnia sticks
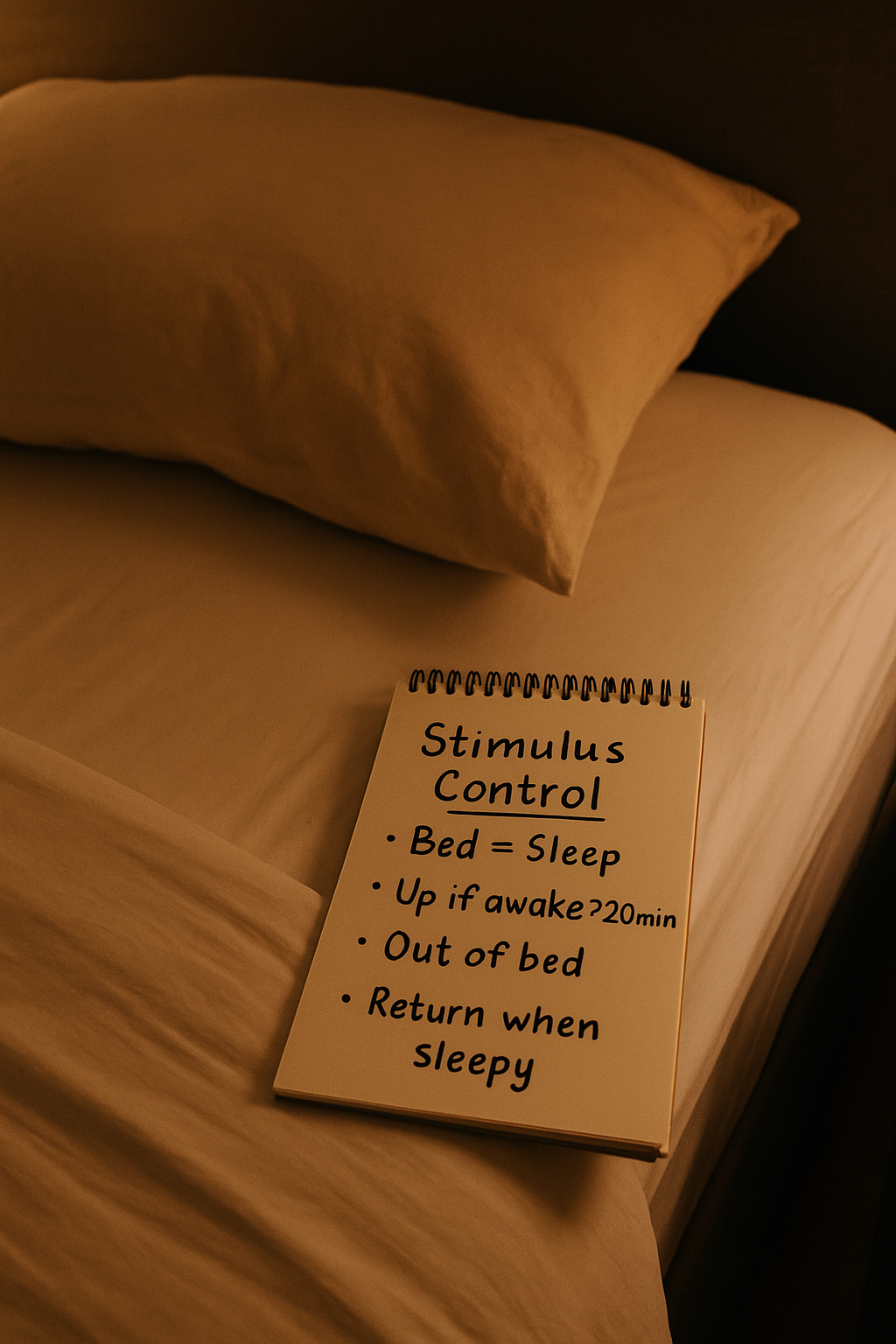
Conditioning: bed becomes linked with struggling instead of sleep.
Hyperarousal: worry and body tension keep the “threat” system up.
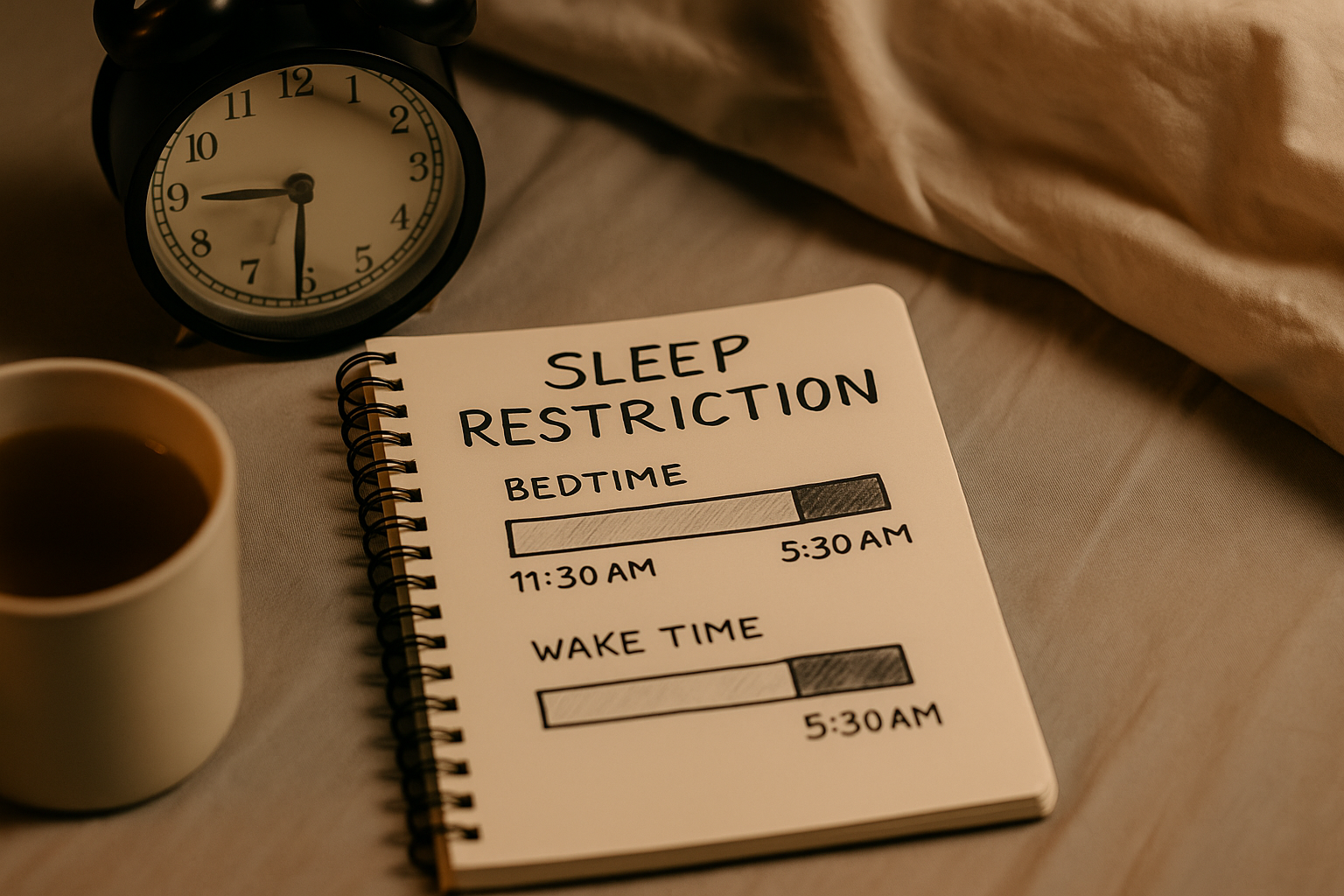
Catch-up naps/lie-ins reduce pressure → another bad night → loop.
Aim to align high sleep pressure with your circadian “sleep gate”.
2) Wind-Down (30–90 min, your way)
Make a dimmer-switch routine: power-down → soothe body → quiet mind.
Power-down: set an alarm to stop tasks; park tomorrow’s 3 bullets.
Mattress & pillows: neutral spine; side-sleepers often need thicker pillow.
Declutter the sightline: fewer “work cues” reduces arousal.
Phones: charge out of reach; use a dumb alarm or Do-Not-Disturb.
8) Naps & Jet Lag
Smart naps
Power-nap 10–20 min (set an alarm). Longer → sleep inertia grogginess.
Keep naps pre-2 pm if you’re trying to fix insomnia.
Jet lag quick plan
Eastbound (earlier clock): morning light at destination; avoid late light; consider low-dose melatonin early evening for a few nights (ask your pharmacist/GP first).
Nightmares/flashbacks linked to trauma that aren’t easing.
Mania history or bipolar disorder (get advice before sleep restriction).
Sleepiness impacting driving/safety — do not drive.
Important Note
The information on this page is for general understanding and support. It is
not a substitute for professional medical, psychological, or legal advice. If you feel
unable to keep yourself safe or someone else is at risk, call 999 (UK) immediately.
If you’re outside the UK, contact your local emergency number.
For non-emergency concerns, consider speaking with a qualified health professional or one of the
support services listed on our site.